What changes
One OPD layer across departments.
Registration, triage, consultation, lab, pharmacy, patient messages, and review stay accountable.
Live demo
See Co Doctor on one OPD case.
For hospitals
Co Doctor connects outpatient registration, doctors, nurse triage, LIMS, pharmacy, patient communication, follow-up, admin controls, audit, and integration readiness around the clinical visit.
Hospital lens
OPD
doctor-led workflow with admin control, role workspaces, audit, and integration boundaries.
What changes
Registration, triage, consultation, lab, pharmacy, patient messages, and review stay accountable.
Money
Follow-up, report review, lab, pharmacy, and patient communication stay tied to the visit.
Quality
Doctor approval, role ownership, audit, and integration boundaries remain visible.
Jump to proof
Purchase proof
The hospital sales case has to prove control: departments keep their surfaces, the HMS is not blindly replaced, and every checkpoint can be inspected by owner.
Revenue
Follow-up, report review, lab, pharmacy, and communication remain tied to the consultation instead of leaking away.
Governance
Provider registry, staff roles, templates, feature flags, audit, and integration boundaries remain visible.
Departments
Collection, report upload, dispense, decline, exceptions, and return-to-doctor status stay attached to the visit.
Quality
Reports, vitals, adherence, recovery summary, fulfilment status, and follow-up completion become reviewable signals.
The shift
Hospitals already have systems that store events. Co Doctor connects those events into a doctor-led pathway with checkpoints, department ownership, audit, and follow-up readiness.
Prescription-based OPD
Treatment-based OPD
Checkpoint economics
For hospitals, the business case is not only doctor speed. It is retained OPD patients, fulfilled services, accountable departments, and auditable continuity.
Consult complete
Revenue
Lab, pharmacy, review timing, and patient communication remain tied to the hospital visit.
Quality
Doctor-approved diagnosis, Rx, orders, advice, and red flags become the continuity source.
Department action
Revenue
Pending reports, dispense status, exceptions, and delays become visible before service leakage compounds.
Quality
Admin and clinical leadership can see where the pathway breaks and who owns the next step.
Continuity review
Revenue
More relevant OPD patients return inside the hospital pathway with reports and recovery context.
Quality
The doctor reviews fulfilment, adherence, patient response, and recovery before changing the plan.
Business case
Hospitals need more than a doctor AI feature. They need measurable continuity across registration, triage, consultation, lab, pharmacy, patient communication, and review.
Leak today
OPD patients leave the hospital pathway after first consult
Checkpoint
Retention and review completion
Evidence to inspect
How many relevant cases receive follow-up timing, reminders, report return, and completed review.
Leak today
Lab and pharmacy services are operationally disconnected
Checkpoint
Order fulfilment visibility
Evidence to inspect
Whether collection, report upload, dispense, decline, and exceptions are visible against the same visit.
Leak today
Admins cannot see where OPD continuity breaks
Checkpoint
Department handoff audit
Evidence to inspect
Queue pressure, pending handoffs, report delays, pharmacy status, and completion readiness by owner.
Leak today
Integration projects drift without proof
Checkpoint
Scoped integration proof
Evidence to inspect
A documented boundary for EHR push, printing, WhatsApp, reports, audit, and data flow before scale.
Why this wins
A hospital buyer needs proof that Co Doctor is not a loose AI screen. It has to sit around the OPD pathway, respect existing systems, and make department leakage visible.
Stops losing
Follow-up, reports, lab, pharmacy, and communication stay connected to the visit instead of falling out of the hospital pathway.
Captures
Reception, nurse, doctor, lab, pharmacy, admin, and patient communication each have owned actions against one connected state.
Closes sale
Admins can inspect roles, templates, audit, integration boundaries, handoff status, exceptions, and review completion.
Next step
The fastest hospital sale is one patient moving through registration, nurse, doctor, lab, pharmacy, communication, and review with ownership visible.
One pathway where reports or pharmacy status go missing
One governance concern around roles, audit, or templates
One HMS/EHR boundary that must stay clear
Buyer questions
That is the hospital buying question. Co Doctor has to connect departments, preserve governance, and make OPD leakage measurable.
Not necessarily. Co Doctor can operate as the OPD clinical and workflow layer, then connect to existing systems for EHR push, reports, printing, WhatsApp, and defined integration needs.
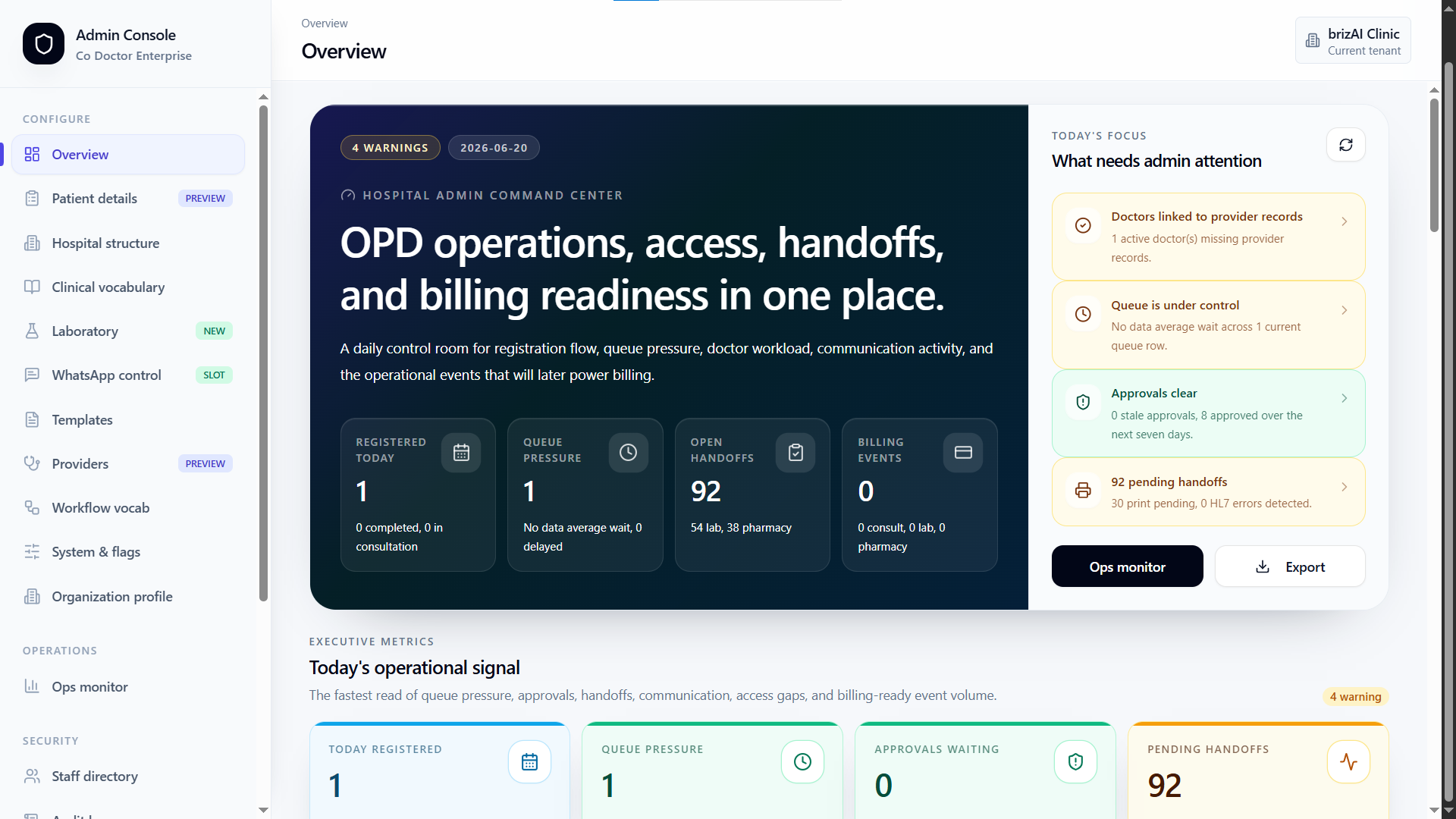
The admin console covers staff directory, provider registry, hospital structure, roles, templates, feature flags, integrations, audit, and operational readiness.
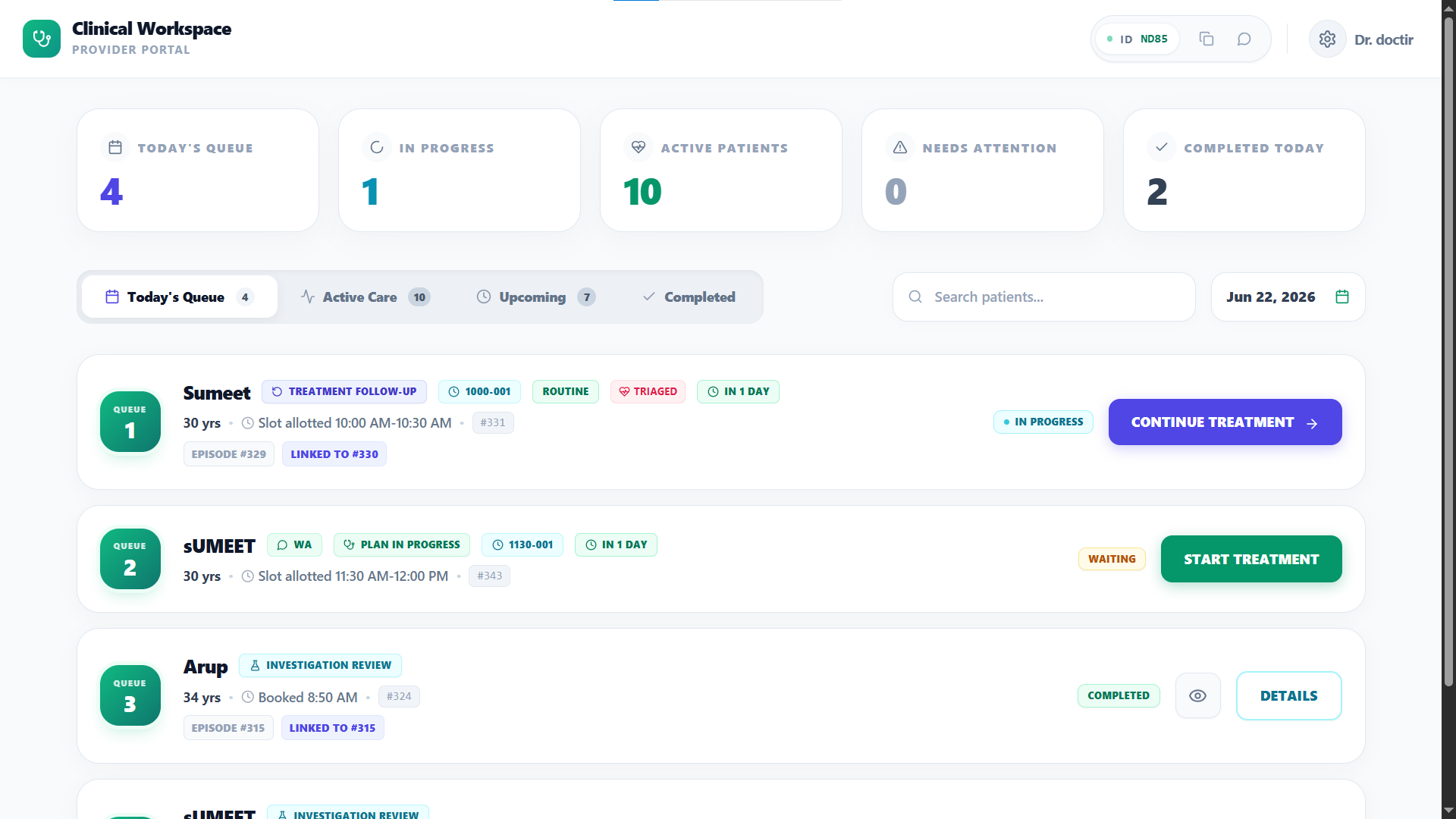
Reception, nurses, doctors, lab, pharmacy, and patient-facing communication each get their own work surface while the visit remains connected.
What stays familiar
The sales case is an OPD operating layer with clear boundaries, not a risky rip-and-replace project.
HMS / EHR
Co Doctor can sit around the OPD pathway and push defined outputs where the hospital wants integration.
Departments
Reception, nurse, lab, pharmacy, doctor, admin, and patient communication get role-specific work without losing one patient state.
Governance
Roles, templates, feature flags, audit, provider registry, and integration boundaries are part of the product story.
One case path
A hospital admin should see one patient cross departments while admin, clinical, and integration boundaries remain inspectable.
Registration
Queue, doctor assignment, patient identity, and visit reason start the connected OPD state.
01
Doctor
Clinical Synthesis, diagnosis, Rx, orders, advice, and review timing are approved in the doctor workspace.
02
Departments
Collection, reports, dispense, decline, exceptions, and return-to-doctor status remain visible.
03
Governance
Admin and clinical leadership can inspect roles, audit, patient response, fulfilment, and review completion.
04
Workflow
Doctor, staff, patient, and admin work off the same treatment loop.
Providers, staff, roles, locations, templates, feature flags, vocabulary, integrations, and audit readiness are configured centrally.
The hospital can add operational depth without making doctors work across disconnected registration, lab, pharmacy, and messaging tools.
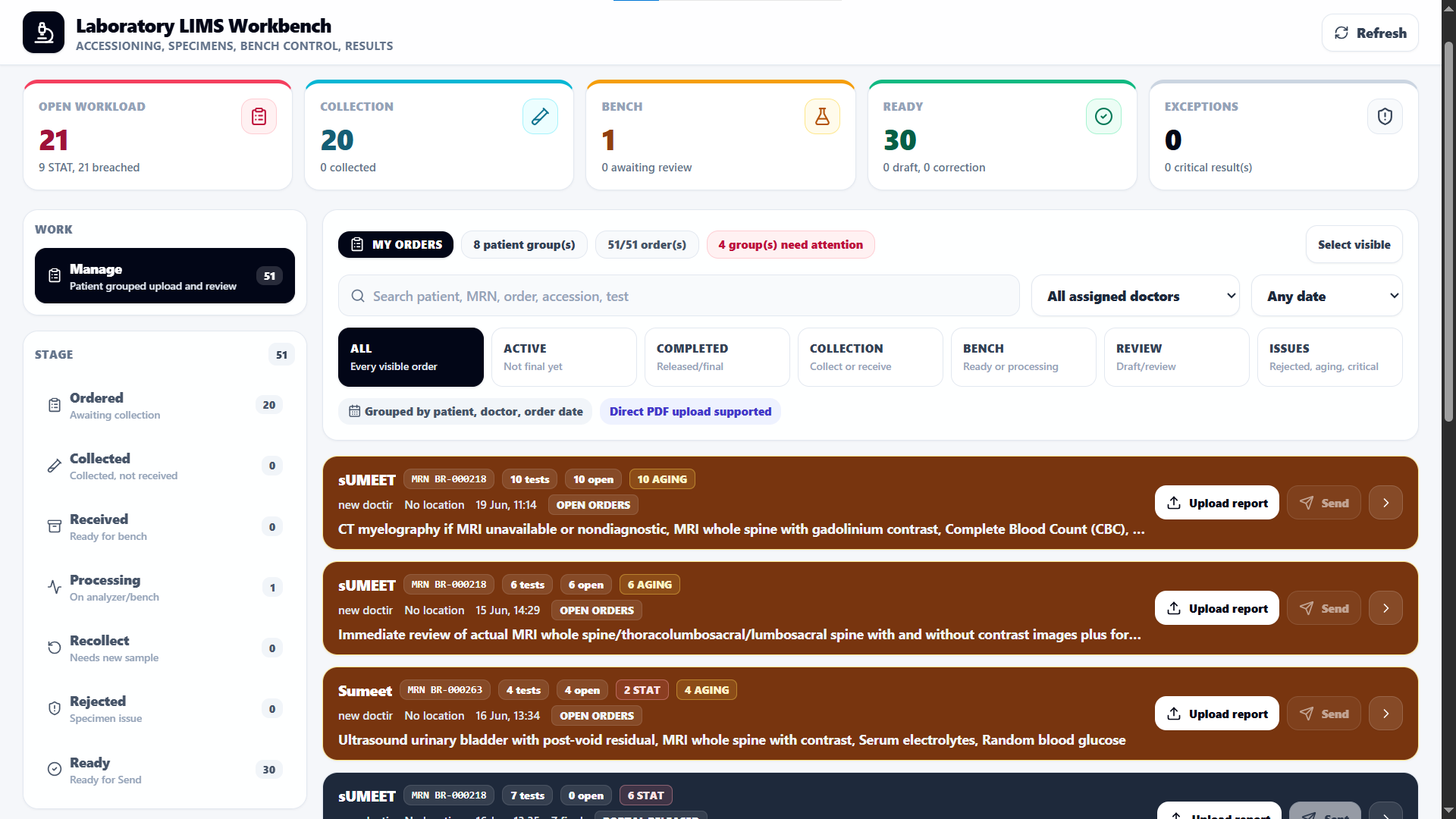
LIMS and pharmacy surfaces track collection, processing, report upload, dispense, decline, exceptions, and return-to-doctor review.
Role access, tenant boundaries, audit trail, integration configuration, and clinical approval rules stay visible.
Buyer map
A hospital buyer needs more than doctor convenience. Each stakeholder needs proof that the OPD layer is governable, useful, and integration-aware.
Hospital admin
Cares about
Provider setup, role control, department ownership, audit, service capture, and OPD leakage visibility.
Proof needed
Inspect admin console, role setup, queue pressure, handoffs, exceptions, and completion readiness.
Clinical leadership
Cares about
Doctor control, review quality, red flags, report context, adherence, and continuity of decisions.
Proof needed
Review one returning patient with previous plan, reports, fulfilment, response, and recovery summary.
IT / operations
Cares about
HMS/EHR boundaries, access rules, auditability, templates, departments, and data flow before scale.
Proof needed
Inspect integration boundaries, tenant/role assumptions, EHR push scope, printing, WhatsApp, and report flow.
Who wins
Less chasing, cleaner handoffs, more patients completing the next step.
Hospital admin
Before
Provider setup, roles, templates, audit, and integrations are hard to connect to OPD outcomes.
With Co Doctor
Controls staff, providers, roles, feature flags, integrations, and readiness around the OPD workflow.
Departments
Before
Reception, nurse, lab, pharmacy, and patient communication complete tasks in separate queues.
With Co Doctor
Each department sees owned work while the visit keeps one connected clinical and operational state.
Clinical leadership
Before
Quality review depends on scattered notes, reports, and delayed feedback.
With Co Doctor
Reviews continuity signals: red flags, reports, fulfilment, patient response, and follow-up completion.
Money and quality
More completed treatment loops, fewer lost handoffs, and stronger review context.
+retention
Case-specific reminders, report return, and follow-up prompts reduce leakage after the first consultation.
+service capture
Lab and pharmacy fulfilment are connected to the visit, making service completion easier to monitor.
+capacity
Clinical Synthesis and repeat draft patterns reduce time spent reconstructing the story in busy OPD.
Operational auditability
Admin can inspect handoffs, exceptions, queues, and completion readiness across teams.
Clinical review quality
Reports, vitals, adherence, response, and recovery summaries come back to the doctor workspace.
Governed automation
Completion actions are configured and doctor-approved, not autonomous treatment decisions.
Product proof
Proof checklist
A hospital needs proof of control, integration boundaries, department ownership, and clinical continuity.
Can admin control staff, providers, roles, templates, feature flags, audit, and integration boundaries?
Can one patient move through reception, nurse, doctor, lab, pharmacy, communication, and review with one connected state?
Are lab reports, dispense status, exceptions, reminders, and follow-up visible by department owner?
Can clinical leadership inspect red flags, fulfilment, patient response, recovery summary, and review completion?
Follow-up engine
Co Doctor turns the treatment plan into owned checkpoints: who follows up, what data comes back, and when the doctor reviews.
Provider setup
Admin
Provider registry, staff directory, roles, templates, integration settings, and readiness are configured.
OPD consult
Doctor
Clinical Synthesis, diagnosis, prognosis, prescription, orders, and next step are approved in one workspace.
Department fulfilment
Lab / pharmacy
Collection, reports, dispense, decline, exceptions, and return-to-doctor status stay attached to the visit.
Continuity review
Hospital OPD
Patient response, report return, reminders, and follow-up completion become measurable OPD signals.
Concerns
Clear boundaries: what changes, what stays doctor-controlled, and what proves value.
Concern
Co Doctor can sit as the OPD clinical and follow-through layer. Replacement is not the default claim; integration boundaries are defined clearly.
Concern
The clinical rule is doctor approval. The admin rule is role control, auditability, configured completion actions, and visible department ownership.
Concern
Co Doctor gives departments work surfaces while tying their output to the visit: lab reports, pharmacy fulfilment, patient messages, and follow-up return to the doctor story.
Concern
The budget case is OPD retention, service capture, doctor capacity, fewer handoff leaks, better report review, and measurable follow-up completion.
Hospital promise
Co Doctor is an OPD operating layer: doctor-friendly at the point of care, but serious about admin control, departments, integrations, and governance.
Ask on WhatsAppQueue pressure, handoffs, lab/pharmacy status, and readiness issues surface earlier.
Providers, roles, templates, integrations, audit, and readiness stay visible.
Reports, medicines, patient replies, and follow-up stay attached to the visit.